Brow Ptosis: Drooping Eyebrows, Foreheads and Brow Lifting
Brow Ptosis- What is it?
Changes in position and shape of the eyebrow are an integral part of facial expression and influence the way in which one's mood and personality are interpreted by others.
Although, there are a variety of eyebrow shapes, on average the female brow has a higher arch than the flatter male counterpart.
With age, the eyebrow starts to descend and become less prominent due to atrophy of the surrounding supporting tendons and deflation of the tissue through loss of fat of the scalp, forehead and temples.
The eyebrow also starts to alter shape and become less stable. A commonly seen feature is descent of the outer tail of the eyebrow with loss of the gently flared shape of youth to become 'comma' shaped. This is commonly referred to as 'clipping' of the eyebrow.
What Causes Brow Ptosis | Drooping Eyebrows
- Normal AgeingMost patients do not notice nor complain of actual descent of the eyebrow at all but increased upper eyelid bags or hooding (dermatochalasis) due to increased redundancy of skin in the upper eyelid fold. For patients wishing to look younger, corrective eyelid surgery (blepharoplasty) will help a lot of these patients but a significant proportion of patients will also require surgery to stabilise or lift the eyebrow. since eyelid surgery alone may actually worsen the pull down further an already drooping eyebrow.
- Certain IllnessesIn addition to normal ageing of the surrounding supporting structures of the eyebrow causing brow ptosis, some disease conditions can cause descent of the eyebrow e.g. facial nerve damage
- Show More


Before and immediately after combined brow lifting surgery combined with ptosis correction surgery. This lady's eyelids and eyebrows were so droopy that it compromised her vision and as such was therefore funded by the NHS for functional reasons.
How Does Brow Ptosis | Drooping Eyebrows Affect You?
- CosmeticPatients complain that they look tired, stern and melancholic
- Headachesfrom fatigue of the forehead muscles as patients try to constantly work to lift up their drooping eyebrows
- Visual Field Compromisesometimes eyebrow descent results in marked redundancy of the below eyelid skin and vision obscuration
- Show More
Brow Ptosis Treatment
Depending on the patient's complaints and brow ptosis severity, various procedures may be performed to improve the stability and position of the eyebrow.
For the small proportion of patients whose symptoms and signs are very severe, these procedures may be offered for functional reasons and would therefore be available on the NHS and through private medical insurance.
However, for most patients who seek treatment for brow descent purely for cosmetic reasons, treatment falls into the realms of cosmetic surgery and is therefore only available privately via self funding.
There are several treatment methods that Mr Cheung offers for the treatment of brow descent/instability, all with a different role to play.
These range from:
- default_titleSimple, non surgical methods e.g. muscle relaxing injections into the tail of the eyebrow using botulinum toxin (Botox®) or injection of dermal fillers into the eyebrow to alter brow shape/position
- default_titleMinimally invasive techniques often used in conjunction with eyelid surgery e.g. transblepharoplasty brow lifting, internal browpexy, orbicularis depressor excision
- default_titleConventional endoscopic and non endoscopic forehead lifting
- default_titleExcisional techniques e.g. direct brow lifting, direct forehead lifting, pretrichial brow lifting, coronal forehead and eyebrow lifting
- Show More
These procedures vary in complexity, postoperative recovery time, procedure duration and permanence. Mr Cheung will be able to counsel you on what is most suitable for you based on what you want to achieve and your personal circumstances.
Brow lift surgery can be performed under:
- default_titleLocal anaesthesia using just numbing injections usually performed by Mr Cheung
- default_titleLocal anaesthesia with conscious sedation. An anaesthetist administers a trickle of sedating medication through the patient's vein to keep the patient relaxed, comfortable and often unaware of the the procedure.
- default_titleGeneral anaesthesia
- Show More
Most brow lift operations are performed as a daycase procedure, that is, the patient goes home the same day. However, some patients prefer to stay overnight in the hospital or nearby hotel especially if they are from out of town.
There is a variety of brow lifting operations, all with different advantages and disadvantages. These will be discussed with you and the most appropriate one for you and your circumstances will be chosen. These include:
- default_titleMinimally Invasive Brow Lifting Techniques
- default_titleConventional Internal Brow Lifting Techniques
- default_titleExcisional Brow Lifting Techniques
- Show More
Minimally Invasive Brow Lifting
Orbicularis depressor excision, internal browpexy and transblepharoplasty brow lifting
These are relatively simple procedures which are usually performed at the same time as upper eyelid cosmetic surgery (blepharoplasty). They have the advantage of being minimally invasive, using the same incision as the eyelid operation, hidden and invisible within the natural skin crease. Thus there are no additional scars and the recovery time is often very, very quick.
Orbicularis depressor excision involves removing a tiny strip of orbicularis muscle which attaches to the tail of the eyebrow causing it to depress. Removing this little strip weakens the depressor action of the orbicularis muscle, allowing the eyebrow tail to elevate slightly.
Internal browpexy involves elevating the eyebrow by releasing from the underlying tissue and securing it to the periosteum (lining of the bone) of the forehead using a suture. This is relatively quick to perform and is fairly inexpensive. Although an internal browpexy does not elevate the eyebrow substantially, it is often very useful in stabilising the eyebrow, allowing safe blepharoplasty surgery.
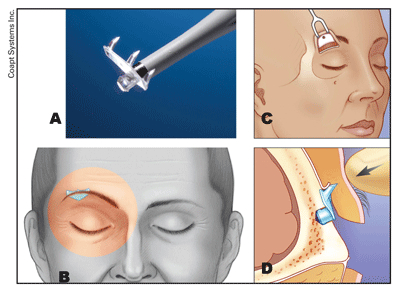
The bone underlying the eyebrow is gently exposed and a tiny partial thickness hole is made in the outer layer of it. The implant is then engaged into this hole. Three hooks on the 'Endotine' transblepharoplasty implant engage the overlying soft tissue of the eyebrow and prop up the eyebrow. The implant the provides a secure convenient support for the eyebrow and overlying forehead tissues and slowly dissolves away over the next 3-4 months to become impalpable.
-

Bilateral lid hooding and brow ptosis: Before bilateral upper lid blepharoplasty and transblepharoplasty brow lifting. This lady was complaining of very heavy eyebrows, headaches and constriction of her peripheral vision.
-

After bilateral upper lid blepharoplasty and transblepharoplasty brow lifting. Notice the improved eyebrow position and shape. Previously the outer tails of her eyebrows were droopy. With a combined brow lift and blepharoplasty, both her eyebrows and eyelids assume a better shape and no longer compromise her visual field. Blepharoplasty surgery alone would not have sufficed.
-

Before Surgery: Upper lid hooding and Brow Ptosis. This lady complained of hooding of her upper lids. Her eyebrows were so unstable, that eyelid surgery on its own would have resulted in further descent of the eyebrow.
-

1 week following internal browpexy and blepharoplasty surgery. The eyebrow was therefore stabilised by using a suture to secure it to the underlying lining of the forehead bone (internal browpexy). Notice that even after only 1 week, much of the postoperative swelling has already disappeared.
-

This lady complained of upper lid hooding on both sides but with the right worse than the left. Note her right eyebrow is lower than her left
-

This lady complained of upper lid hooding on both sides but with the right worse than the left. Note her right eyebrow is lower than her left
-

1 week following blepharoplasty surgery to both upper eyelids and elevation of her right eyebrow to match the other side using an endotine transblepharoplasty implant. Note the perfect symmetry of her eyebrows and eyelids again
-

All incisons are hidden with the normal skin creases
-

….which have almost vanished at 6 weeks following surgery.
-

Before surgery again
-

After surgery again
-

This lady complained of marked hooding of her eyelids. Notice that her eyebrows are also quite low and rounded on the ends (brow ptosis). Unfortunately blepharoplasty surgery alone would likely cause further descent of the eyebrow and would be insufficient.
-

This lady complained of marked hooding of her eyelids. Notice that her eyebrows are also quite low and rounded on the ends (brow ptosis). Unfortunately blepharoplasty surgery alone would likely cause further descent of the eyebrow and would be insufficient.
-

1 week following bilateral upper lid extended blepharoplasty with internal browpexy. The internal browpexy stabilises the eyebrows and stops them from descending further. The blepharoplasty itself has had to be extended outwards into one of the lateral crow's feet to address the lateral hooding of the eyelids
-

1 week following bilateral upper lid extended blepharoplasty with internal browpexy. The internal browpexy stabilises the eyebrows and stops them from descending further. The blepharoplasty itself has had to be extended outwards into one of the lateral crow's feet to address the lateral hooding of the eyelids
-

1 week following bilateral upper lid extended blepharoplasty with internal browpexy. The internal browpexy stabilises the eyebrows and stops them from descending further. The blepharoplasty itself has had to be extended outwards into one of the lateral crow's feet to address the lateral hooding of the eyelids
-

6 weeks after surgery, most of the wounds have disappeared leaving a tiny degree of skin redness of the crow's feet which continue to fade away over the next 3 months
-

6 weeks after surgery, most of the wounds have disappeared leaving a tiny degree of skin redness of the crow's feet which continue to fade away over the next 3 months
-

6 weeks after surgery, most of the wounds have disappeared leaving a tiny degree of skin redness of the crow's feet which continue to fade away over the next 3 months
-

Before surgery again
-

After surgery again
Endoscopic and non endoscopic internal brow and forehead lifts
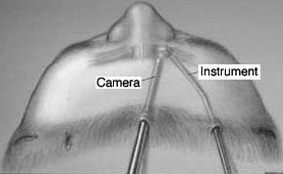
An internal brow lift is often used in middle aged patients with moderate amounts of brow ptosis. Although originally used in cosmetic surgery, internal forehead lifts with or without the aid of an endoscope has been used successfully in patients with mild functional brow ptosis due to certain diseases e.g. facial nerve palsy. Not only does it elevate the eyebrow, it also smooths out the forehead wrinkles. These internal brow and forehead lifts involve the release of the the descended forehead and eyebrow off the underlying bone of the forehead, sometimes with the aid of a rigid endoscope. Five small incisions behind the hairline are performed to allow release of the upper forehead to allow dissection of the retaining ligaments of the forehead soft tissues. These incisions heal to leave fine scars hidden within the hair. The tissues are then elevated and secured using a variety of fixation techniques. In addition to being able to release the retaining ligaments of the forehead and brow, an internal brow lift also allows for partial removal of some of the wrinkle and furrow causing muscles of the eyebrow and bridge of the nose.
Many surgeons are now recognising that the newer more reliable fixation techniques to elevate the eyebrow and forehead can also be employed e.g. endotine forehead fixation devices, without the cost and morbidity associated with performing a full internal forehead lift using an endoscope. In addition, many feel that the extreme amounts of lift associated with such extensive forehead dissection often result in an unnatural eyebrow giving a surprised, windswept look and that what is more important now is more subtle recontouring of the eyebrow shape instead i.e. less is more.
Overall Mr Cheung will tend to reserve this technique when there is generalised mild to moderate drooping of the eyebrow. For the more commonly seen temporal brow droop i.e. descent of the tail of the eyebrow, Mr Cheung prefers newer less invasive techniques e.g. transblepharoplasty brow lifting.
These operations are not suitable for patients with a high hairline due to scalp incisions. Patients can usually return back to normal activities 2 weeks following surgery.
Direct brow lift, temporal (pretrichial) lift, direct forehead lift and coronal brow lifts
Although these techniques of brow lift have been around the longest, they still have a significant role to play in modern surgery. They all have in common the fact that they are excisional techniques, where a strip of tissue above the eyebrow to be lifted is excised (removed). Because of this, they allow for significant amounts of brow lifting and are still considered to be the longest lasting of all the brow lifting techniques. The main disadvantage of excisional techniques is that a skin scar is created. However, the scar often becomes inconspicuous/ invisible.
For these reasons, excisional techniques have a major role to play in severely drooping eyebrows/foreheads often due to pathological conditions e.g. damage to the nerves supplying the facial muscles, where significant reliable amounts of lifting are commonly necessary.
- default_titleDirect brow lift involves the removal of skin just above the eyebrow and is mainly used in older patients or patients with severe brow ptosis, commonly due to facial nerve damage. The incision scar will often look like normal forehead wrinkles in time or disappear outright. A direct brow lift not only has the advantage of being the most effective and predictable method of lifting a ptotic eyebrow, but also has the side effect of smoothing out the forehead furrows slightly by pulling it downwards towards the eye. This leads to an ironing out the forehead furrows and a pulling down of the hairline slightly, which is particularly useful in patients with a high hairline. Care is taken to try and hide the incision just above the eyebrow hairs.
- Show More
-

Direct Brow Lifting: This patient has a drooping eyebrow due to paralysis of the facial nerve
-

Direct Brow Lifting involves removing a small slither of skin above the eyebrow. Here the required amount of skin has been marked out ready for removal.
-

Direct brow lifting: A fine scar may remain following surgery but for most patients this is cosmetically acceptable
- default_titleA temporal (pretrichial) brow lift is useful for a patient who requires a moderate lift of the outer aspect of the eyebrow only. The incision is made in the temple just behind the hairline and involves the removal of a strip of hair-bearing skin.
- default_titleDirect forehead lift involves removing a strip of forehead skin and muscle. Usually performed in men older than 50 due them commonly having pre-existing deep forehead furrows, the incisional scar is hidden within a forehead line. Although initially quite visible, the postoperative scar often fades away over time to resemble a normal forehead wrinkle.
- default_titleThe coronal forehead and brow lift is the most invasive approach to brow lifting. This involves a large incision running across the scalp a few centimetres behind the hairline. Although considered outdated, this approach still has a significant role in patients with a marked brow ptosis. The disadvantages of this approach are the scar and potential permanent numbness of the scalp behind the scar which extends to the centre of the scalp.
- Show More
Postoperative Care
After brow lifting surgery, depending on the operation type, pressure dressings may be applied to minimise swelling. These are usually removed by the patient usually within 24 hour of the surgery and the patient is asked to apply ice compresses to reduce swelling further. If there are any stitches then these are usually removed at 7-14 days. Although 80-95% of the swelling has usually dissipated by 2 weeks, some minimal residual swelling may remain at 3-6 months. You may be asked to apply antibiotic ointment to the skin wounds and some ocular lubricants to the eyes, especially if a blepharoplasty operation has been performed as well.
