Epiphora: Watery Eyes
The Normal Tear System
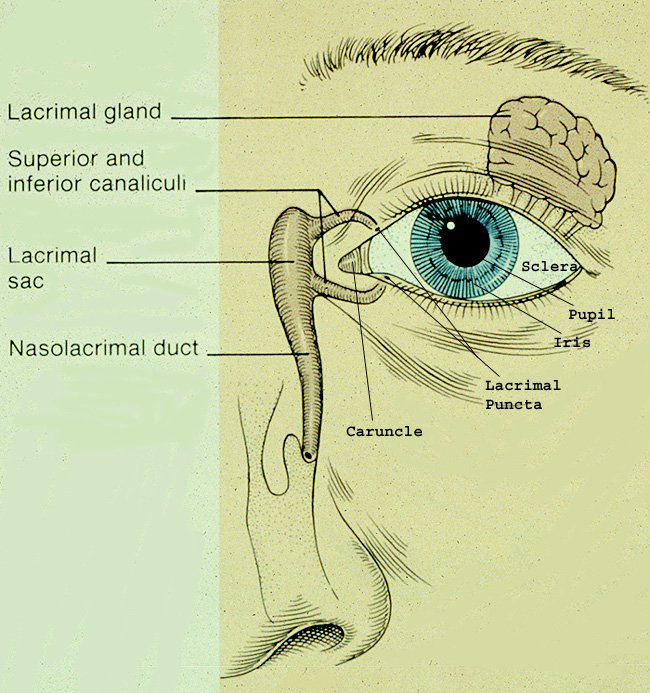
- default_titleThe eye has several tear glands which produce tears on to the surface of the eye, the largest of which is the lacrimal gland, sitting behind the upper lid.
- default_titleTears are important in helping to wash, clean and lubricate the eyeball surface.
- default_titleThe eyelids behave like squeegees; distributing the tear film evenly across the eyeball surface with every blink.
- default_titleThe tears then drain away through small openings (also called puncta) found on the edge of the upper and lower eyelids near the nose. These openings lead into small channels (called canaliculi) , which meet and drain into the tear drainage system within the nose (lacrimal sac and duct).
- default_titleThe tears then empty out of the passageway system within the nose, where they are then automatically swallowed.
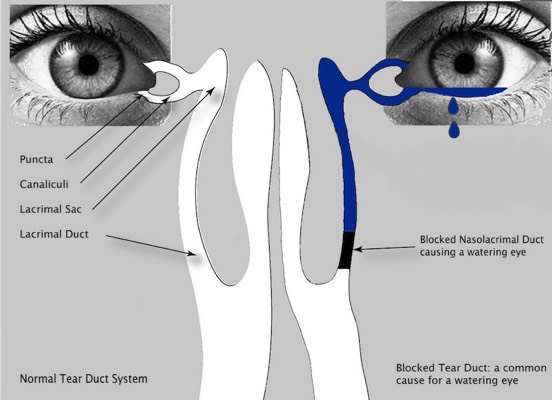
- default_title If the tear duct is blocked your tears back up and spill over your eyelids as if you are crying. Tears trapped in the tear sac also become stagnant and infected.
- Show More
What Causes a Watering Eye?
There are many causes of a watery eye and some patients may have several causes of a watery eye at the same time.
Common causes include:
- default_titleAnything which causes irritation of the eye surface will cause the tear gland to produce more tears (reflex hyperlacrimation). One of the commonest causes is Inflammation of the eyelid edges (called blepharitis or meibomian gland dysfunction)
- default_titleLoosening of the eyelids due to age, reducing their ability to wipe away the tears.
- default_titleAn abnormal eyelid position can also cause a watering eye:
An eyelid which turns inwards (entropion) cause cause irritation of the eye and hence watering due to the discomfort caused.
An eyelid which turns outwards (ectropion) can result in the punctum no longer being in the correct position to collect the tears. - default_titleA narrowing/ blockage of the punctum can prevent tears draining into the tear duct system.
- default_titleA blockage of the tear drainage system within the nose. Blockages at the bottom of the tear drainage system often leads to stagnation and collection of tears with the tear sac, which may then become infected.
- Show More
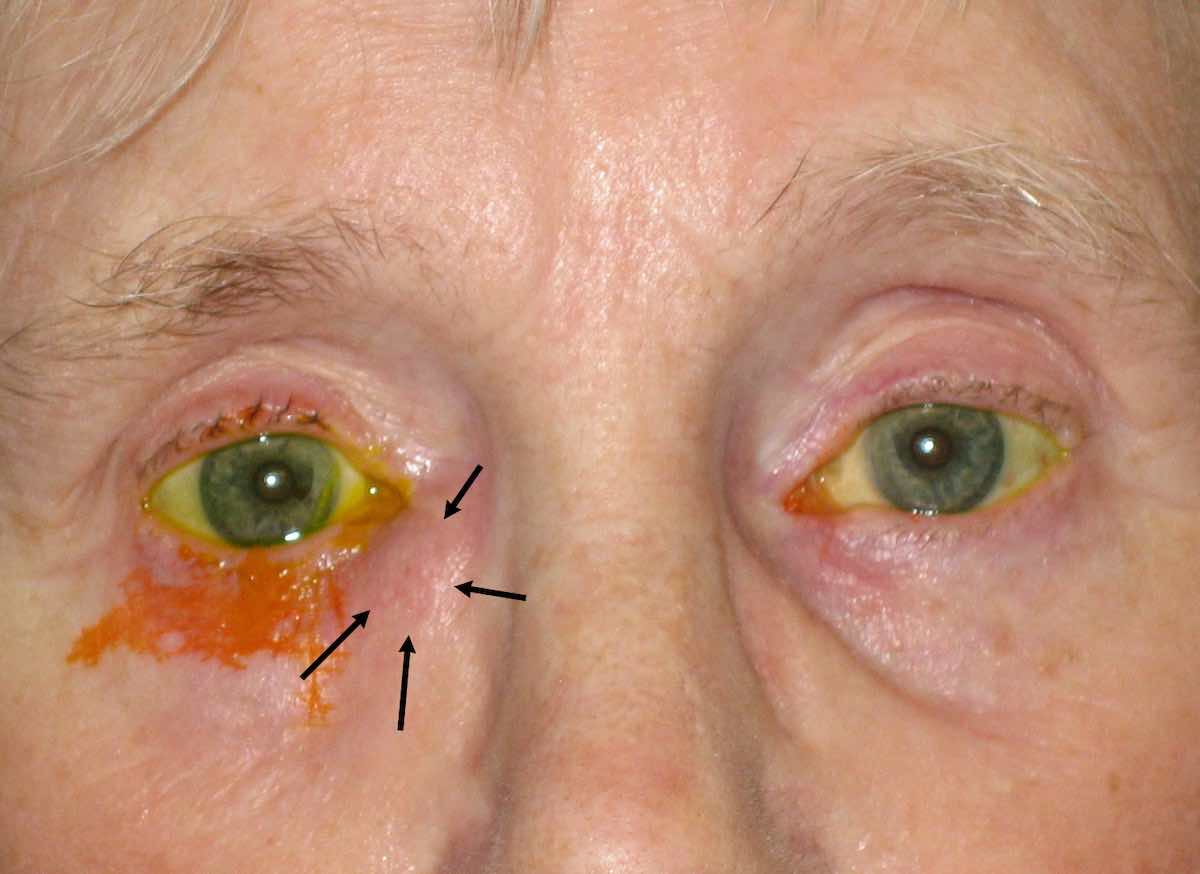
The Fluorescein Disappearance Test in patient with a blocked tear duct: The right (her right) tear duct of this lady is blocked. Yellow dye eye drops (fluorescein) have been put into both eyes at the same time. Note the dye takes much longer to drain away from her right eye and overflow down her eyelid. Note the swelling in corner of the right lower lid. This represents a small collection chronic infection within the tear duct (lacrimal sac mucocoele). As the tears cannot drain away adequately, they become infected.
In summary watering eyes can be due to either the tear gland producing too many tears (hyperlacrimation), often as a result of eye surface irritation for whatever reason) or an interruption in the normal tear drainage pathway or a combination of both. It is therefore important to see an oculoplastic surgeon who will have the tools to be able to diagnose the cause and then be able the correct treatment.
-

Ectropion: note the out turning eyelid. Watering commonly results
-
1 week following ectropion correction surgery.

Chronic infection of the lacrimal sac



Canaliculitis: an uncommon cause of watering eye. This lady had been complaining of a watering eye, swelling of the inner eyelid with sticky irritable discharge arising from the opening of the tear duct (punctum) for six months. Surgery is often required to help resolve the infection

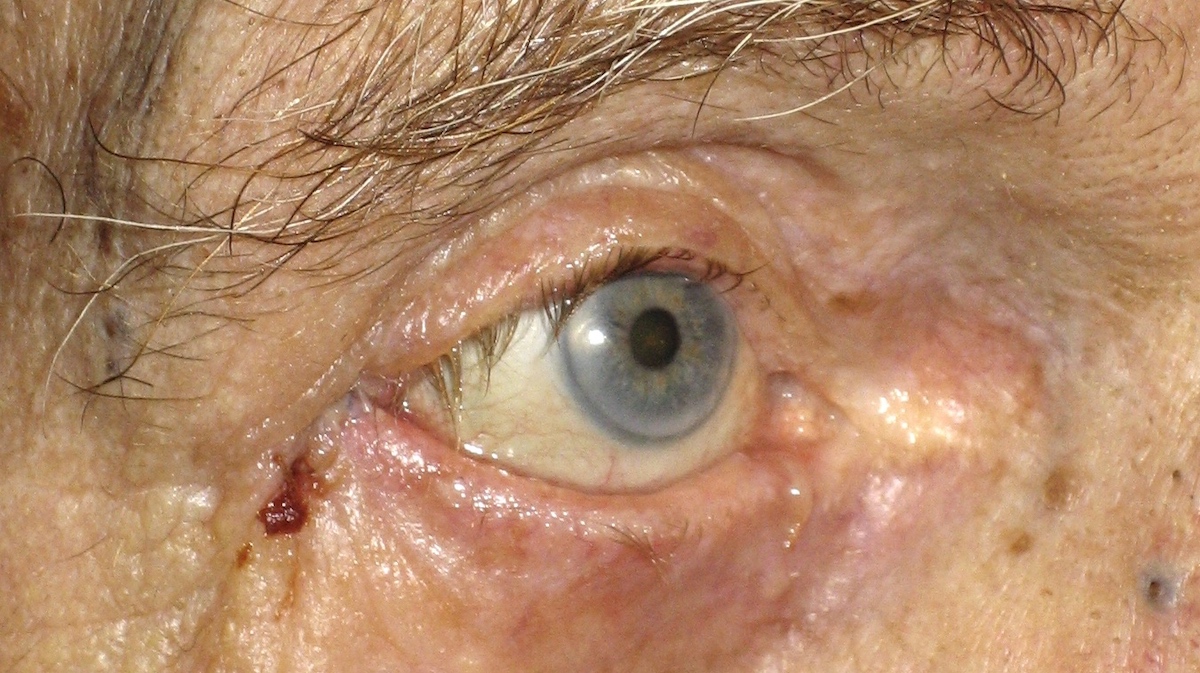
Acquired Lacrimal Sac Fistula (arrowed): An uncommon complication of infection of the tear duct system- sometimes infections of the tear duct and tear sac can rupture through the skin, resulting in a connecting hole. Here yellow fluorescein drops have been instilled into the eye, only for them to enter into the tear drainage system normally but then emerge out through the abnormal hole. The patient complains of tears emerging through the hole constantly.
Blocked Tear Duct Surgery / Dacryocystorhinostomy (DCR)
Obstructions within the lacrimal drainage channels will often require an operation called a dacryocystorhinostomy or DCR for short. This operation has been performed for over 100 years and tends be very successful when performed correctly. However, the chance of success varies from patient to patient and is dependent on various factors including type and site of obstruction, patient symptoms and any previous surgery.
-
The vast majority of patients who suffer from a blocked tear duct systems usually have a blockage located near the end of the system within the nasolacrimal duct.
-
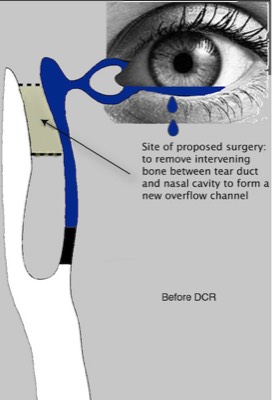
The aim of DCR surgery is to create a new bypass channel so that the tears can pass from the lacrimal sac into the nose again through the new bypass channel; therefore bypassing the blockage within the nasolacrimal duct. Thus the patient no longer has a watery eye since stagnation of tears no longer occurs.
-
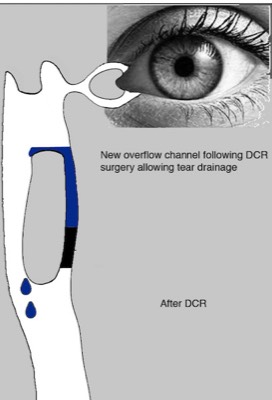
A new bypass channel is created by removing the intervening bone between the lacrimal sac and nasal cavity and then connecting the lacrimal sac to the lining of the inside of the nose.
A small length of soft plastic tubing is threaded through the bypass channel, to help maintain patency of the new drainage system whilst the new bypass channel heals. This is easily removed in the outpatient clinic shortly after the operation (usually within 3 months)
External DCR & Endoscopic DCR
• In the UK, the vast majority of DCR surgery is by external DCR. This is performed through a small cut of the skin on the side of the nose (External DCR). The careful placement of the incision, meticulous wound closure and intensive application of special ointments following surgery means that for 99% of patients, the wound the scar becomes so inconspicuous that patients do not report it to be a cosmetic issue.
• Increasingly, DCR surgery is performed with the aid of a special telescope to look up the nose (Endoscopic DCR). This allows for usually less invasive surgery allowing for quicker patient recovery after surgery and no risk of developing a skin scar.
Currently, success rates for external DCR surgery are greater than endoscopic DCR surgery for all types of blockage. Whether or not surgery can be performed endoscopically is dependent on numerous factors including nasal access and the location of the obstruction.
Mr Cheung performs both types of operation. DCRs are usually performed as a day case procedure meaning that the patient goes home on the same day after surgery. Although, DCRs can be done under local anaesthesia, most patients prefer general anaesthesia
-

1 week following external DCR surgery. Notice the skin incision
-

6 weeks following external DCR surgery. The skin incision wound has become invisible
-

6 weeks following external DCR surgery. The skin incision wound has become invisible
-

6 weeks following external DCR surgery. The skin incision wound has become invisible
-

6 weeks following external DCR surgery. The skin incision wound has become invisible
-

6 weeks following external DCR surgery. The skin incision wound has become invisible